






 Information in English
Information in English















28 May 2003: Yet Another Day of Action for the Health of Women
Ximena Andrade
Published in: Outras Vozes, Suplemento do boletim n° 3, July 2003
This paper marks 28 May, the International Day of Action for Women’s Health, that this year is taking up again its original purpose, by drawing attention to the problem that it wanted to see emphasised as far back as 1988 – the relationship between the patent subordination of women in society and high levels of maternal morbidity and mortality, summarised in the phrase “a maternal death should and must be seen as the culmination of a process that starts the moment a woman is born”.
Box 1
| Region | Nº |
|---|---|
| of deaths | |
| Africa | 273 000 |
| Asia | 217 000 |
| Latin America, Caribbean | 22 000 |
| Europe | 2 000 |
| Oceania | 560 |
| North America | 490 |
| World Total | 515 000 |
Source: Maternal Mortality in 1995: Estimates developed by WHO, UNICEF, UNFPA. World Health Organization, Geneva, 2001
That year, given the serious and deteriorating situation in the world, two international networks of the international women’s movement, the World Network of Women for Reproductive Rights and the Health Network of Latin American and Caribbean Women, decided to launch a campaign to reduce maternal mortality. Consequently, on 28 May they launched an appeal for work to start on raising awareness about the lack of recognition of women’s rights: maternal mortality and morbidity.
Box 2
| resulting maternal morbidity | ||
|---|---|---|
| Heavy bleeding (haemorrhage) | 11% |
|
| Infection during and after birth (septicaemia) | 10% |
|
| Prolonged or obstructed delivery | 6% |
|
| Hypertension caused by pregnancy (preclampsy and eclampsy) | 6% |
|
| Non safe abortion | 16% |
|
% – Incidence (in % of live births)
Source: C. Murray & A. Lopez, eds., Health dimensions of sex and reproduction (1998): chapters 5 to 8
So what was the situation that was denounced then and is still being denounced today? According to the WHO, every year there are 210 million pregnancies. Of the roughly 130 million births each year, about 15-19% require rapid intervention by qualified staff so that a woman can survive and not be incapacitated for the rest of her life. Lethal complications arise in approximately 5% of cases. According to available data, in 1995 it was estimated that over half a million women died from complications during pregnancy, birth or post partum. These tragic figures have been rising despite the fact that in 1987 the WHO and other United Nations and international agencies directly interested in the maternal mortality situation made it a top priority in international public health and proposed the initiative on risk-free motherhood.
Box 3
| Region | Nº | |
|---|---|---|
| of maternal deaths due to unsafe | of death following an unsafe abortion | |
| Africa | 33 000 | 1 in 150 |
| Asia (*) | 37 600 | 1 in 250 |
| Latin America | 4 600 | 1 in 900 |
| Europe (**) | 500 | 1 in 1 900 |
* Excludes Japan, Australia and New Zealand.
** Primarily Eastern Europe/Newly Independent States (NIS)
Source: Abortion: A Tabulation of Available Information 3rd edition, World Health Organization, Geneva, 1998
What proof is there of this?
- Some 1,600 women die every day i.e. almost 600,000 a year, following pregnancy, birth or post partum complications. Of these deaths, 99% occur in underdeveloped countries. But these figures on maternal mortality are only the tip of the iceberg. “For each case of maternal death, at least another 30 women suffer serious or debilitating lesions”. (Ashford: 2002).
- Haemorrhage, infections, hypertension difficulties (eclampsy), obstructed delivery and complications arising from unsafe abortion are the main causes of maternal deaths. In various Third World countries, unsafe abortion is one of the prime causes of maternal mortality. (WHO/OPS: 2002). This is why it is important to emphasise that complications rarely arise in abortions performed by qualified professional. WHO estimates that there are about 18 million risky abortions every year in less developed countries, one for every 10 pregnancies or one for every seven live births” (Murray & Lopez: 2000).
- Some 40% or more of pregnant women – 15 million a year – have morbidity related to gestation, or during or immediately after the birth. 15% suffer serious immediate or long-term complications such as, for example, retroverted uterus, fistula (opening in the delivery channel that permits infiltration from the bladder or rectum into the vagina), pelvic inflammatory disease and infertility (Safe Motherhood Initiative: 2003). (Safe Motherhood Initiative: 2003).
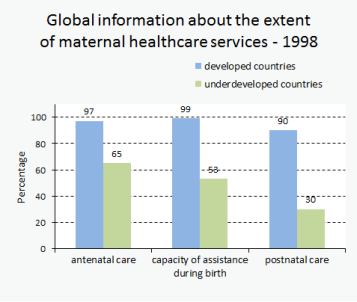
- About 35% of women in underdeveloped countries receive no antenatal care during pregnancy. In some countries antenatal coverage is only 26%. (Safe Motherhood Initiative: 2003).
- Roughly half the births in Third World countries take place without professional care. In some of these countries the rate reaches 85%. (Safe Motherhood Initiative: 2003).
- 70% of women receive no postpartum care in the six weeks following birth. (Safe Motherhood Initiative: 2003).
When we observe this reality at the regional level, data on maternal mortality provided by the World Health Organization highlight the very profound differences between the developed and the underdeveloped world. They provide the strongest indication of the inequity in health faced by women, even though much more is now known about its main causes, and the most appropriate interventions – most of which simple and low-cost – to avoid it have been identified. Here we should consider the reproductive risk index that encompasses the indicators maternal mortality ratio (maternal deaths per 100,000 live births, and total fertility rate (average live births per woman. (Population Action International: 2001 and Population Reference Bureau: 2003) and lifelong risk, i.e. the probability that a woman will die due to complications during pregnancy, birth or a risky abortion throughout her life. (Box 4)1.
Box 4
| maternal mortality risk |
|
|---|---|
| Africa | 1 in 16 |
| Asia (*) | 1 in 110 |
| Latin America and the Caribbean | 1 in 160 |
| Europe | 1 in 2000 |
| North Amercia | 1 in 3500 |
* Excludes Japan, Australia and New Zealand.
Source: Maternal Mortality in 1995: Estimates developed by WHO, UNICEF, UNFPA. World Health Organization, Geneva, 2001
It has been stressed that this serious inequity in health is related to the subordinate position of women in society, where they do not have the necessary power to take free and informed decisions on their sexuality and reproduction. It is also related to the level of development of health systems, the coverage and quality of services, priority in the allocation of resources for preventing maternal mortality and equitable access to good quality health care. This means that the level of economic development of countries is important as well as their priority in allocating resources for prevention and treatment. It is interesting to note that in some countries with a GDP that is not very high maternal mortality rates have fallen because they have known how to allocate their health resources effectively, giving priority to maternal health promotion and prevention measures (ISIS international: 2002)2.
Various ways of addressing this serious health and human tragedy have been presented. They all converge on one common aspect: respect for the human rights of women and a commitment to cultural, economic and social changes that improve their status and permit their real empowerment. In addition, from the health point of view the provision of qualified care during birth, increased access to and coverage by services and better quality care are priority steps towards exercising the rights of women who will become mothers. Effective interventions to address the costs of primary health care are also fundamental in the fight against maternal mortality.
Which of a woman’s human rights are compromised by maternal mortality? The purpose of this topic is to open a debate that identifies proposals on actions aimed at law reform and to improve and/or prepare proposals on public policies. The prevention of maternal mortality and morbidity encompasses various non-hierarchical areas of women’s human rights in that, by definition, human rights are inseparable within a systemic whole. They are: the right to life, sexual rights, reproductive rights, access to health and education and the right to live a life without violence, among others.
What have the women’s movement and the feminist movement achieved in terms of preventing maternal mortality and morbidity?
The human rights of women linked to preventing maternal mortality and morbidity have been expressed in various international legal instruments ever since Maternal Health: a Human Right started to be addressed. The need to protect maternal health has been recognised in various international documents such as the Action Programme of the 1994 Cairo International Conference on Population and Development, the Action Platform of the World Conference of Women in Beijing in 1995, among others. The Development Objectives for the Third Millennium established by the United Nations and the World Health Organization also emphasise the urgent need to reduce the high rates of maternal mortality. Objective 5, “Improving Maternal Health.
What is the situation in Mozambique? We should start by noting that health services only cover approximately 40% of the country. The only information available on maternal mortality is the inter-hospital figures that are equivalent to only 28-40% of all births each year.
In the country as a whole and in the various regions, the maternal mortality rates in 1999, 2000 and 2001 were as follows:
Unit199920002001
| Territorial | |||
|---|---|---|---|
| National | 1 540 | 1 750 | 1 650 |
| North | 1 870 | 2 660 | 2 020 |
| Center | 1 880 | 1 750 | 1 720 |
| South | 970 | 1 000 | 1 220 |
| Maximum values: Cabo Delgado | 4 340 | 5 120 | 4 090 |
| Minimum values: Maputo City | 440 | 450 | 600 |
The following table compares the situation in Mozambique with other parts of the world, using some ad hoc key indicators:
UnitPrevalence
| Territorial | of contraceptives (%) 1995 – 2000 | % births assisted by trained health staff 1995 – 2000 |
|---|---|---|
| Mozambique | 10 | 44 |
| African Countries South of the Sahara | 18 | 37 |
| Middle East and North Africa | 49 | 69 |
| Southern Asia | 40 | 29 |
| East Asia and the Pacific | 81 | 66 |
| Latin America and Caribbean | 69 | 83 |
| Industrialised Countries | 72 | 99 |
| Developing Countries | 59 | 52 |
| Less Developed Countries | 24 | 28 |
| World wide | 64 | 56 |
Finally, we should not forget that in addition to reproductive and sexual rights (the ones related to maternal mortality and morbidity) many other issues related to the position of women in gender relations are detrimental to their health. For example, women are at greater risk than men of being infected by the HIV virus in sexual encounters; pregnant women are more likely to be victims of domestic violence; women tend to request and receive medical care only when they are seriously ill. In recent years the feminist movement has called attention to problems linked to maternal mortality and morbidity such as: violence against women; the right to abortion and the corresponding services; sexually transmitted diseases; HIV/AIDS and the need to supply safe and effective contraceptives that are sensitive to women’s needs, not directed by population control policies but based on a vision of a woman’s human rights.
References:
-
Amnesty International: www.es.amnesty.org/temas/mujeres/violencia-contra-las-mujeres
-
UNFPA: www.unfpa.org
-
ISIS International. Health Agenda: www.isis.cl
-
Mujeresred-violencia mailing list: write to Mujeresred-violencia@listas.nodo50.org
-
Population Action International: populationaction.org
-
Population Reference Bureau: www.prb.org
-
Safemotherhood Initiative: safemotherhood.org
-
WHO: www.who.org